Stroke — Ischemic vs Hemorrhagic, FAST, tPA Rules, and Nursing Priorities
April 10, 2026
Test Your Knowledge
12 questions · Audio-based · Study on the go
Stroke: Ischemic vs Hemorrhagic, tPA Rules, and Nursing Priorities
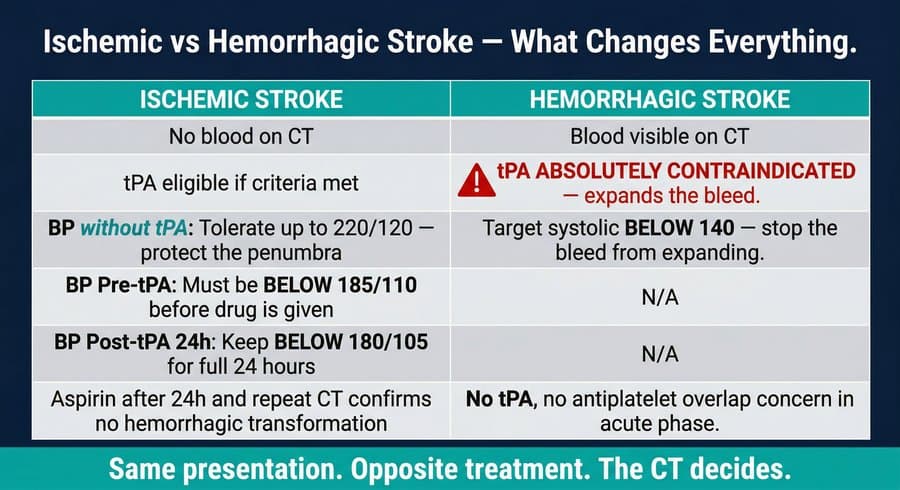
Stroke remains a leading cause of death and long-term disability worldwide. In clinical nursing, no topic demands faster, more accurate decision-making than acute stroke. The central challenge is this: ischemic stroke and hemorrhagic stroke can present with nearly identical symptoms, yet their treatments are not just different — they are opposite. Giving the wrong treatment can convert a survivable event into a fatal one.
Recognizing Stroke: FAST and Last Known Well
The FAST mnemonic captures the four hallmark signs of stroke. F stands for facial drooping — one side of the face droops or goes numb, and the patient cannot produce a symmetric smile. A stands for arm weakness — when both arms are raised, one drifts downward. S stands for speech difficulty — speech is slurred, garbled, absent, or incomprehensible. T stands for time, specifically the time to call emergency services.
The T in FAST carries a clinical detail that is frequently misunderstood. The relevant time is not when symptoms were discovered, when EMS arrived, or when the patient reached the emergency department. It is the time of last known well — the last moment the patient was observed or confirmed to be at their neurological baseline. In a witnessed onset, this is the moment symptoms began. In an unwitnessed onset, such as when a patient wakes up with deficits, last known well is the last time they were confirmed normal, typically when they went to sleep. This distinction determines the entire tPA eligibility window.
The Critical First Step: CT Without Contrast
Ischemic and hemorrhagic stroke cannot be reliably distinguished on clinical presentation alone. Both cause focal neurological deficits. Both typically cause elevated blood pressure. The classic thunderclap headache associated with subarachnoid hemorrhage is characteristic but not universal. A patient who denies headache, reports no vomiting, and presents with a unilateral deficit could be either type.
The consequences of this ambiguity are severe. Alteplase — the thrombolytic agent used in ischemic stroke — works by dissolving fibrin-based clots. In hemorrhagic stroke, the clot at the rupture site is the body's only attempt to stop the bleed. Administering alteplase dissolves that seal, causing hemorrhage expansion, rising intracranial pressure, and often herniation. This is why a non-contrast CT of the head is mandatory before any thrombolytic decision. The CT is not a procedural delay. It is the treatment decision.
Ischemic Stroke and the Ischemic Penumbra
When a cerebral artery is occluded, the tissue at the center of the blocked territory — the infarct core — begins dying immediately. Surrounding it is the ischemic penumbra: brain tissue that is not functioning but is not yet dead. The penumbra is kept marginally perfused by collateral blood vessels that branch around the obstruction. These collaterals are pressure-dependent. They carry blood only because systemic blood pressure is high enough to force flow through narrow alternative channels.
This physiology drives every blood pressure decision in ischemic stroke. Aggressive blood pressure reduction closes those collateral pathways and kills the penumbra, expanding the permanent infarct. Current guidelines therefore recommend a permissive approach to blood pressure in ischemic stroke without thrombolytic therapy, tolerating values up to 220/120 mmHg unless another condition independently requires reduction.
Blood Pressure Targets by Situation
Nurses must know three separate blood pressure targets in stroke care, and they vary by situation. For ischemic stroke not receiving tPA, blood pressure is tolerated up to 220/120 mmHg. For ischemic stroke receiving tPA, blood pressure must be brought below 185/110 mmHg before the drug is administered. Once tPA infusion begins, the ceiling drops to 180/105 mmHg and must be maintained there for the full 24 hours following the infusion. For hemorrhagic stroke, the target is systolic blood pressure below 140 mmHg, because there is no penumbra to protect — the priority is reducing the force driving blood through the rupture.
tPA Eligibility and the Extended Window
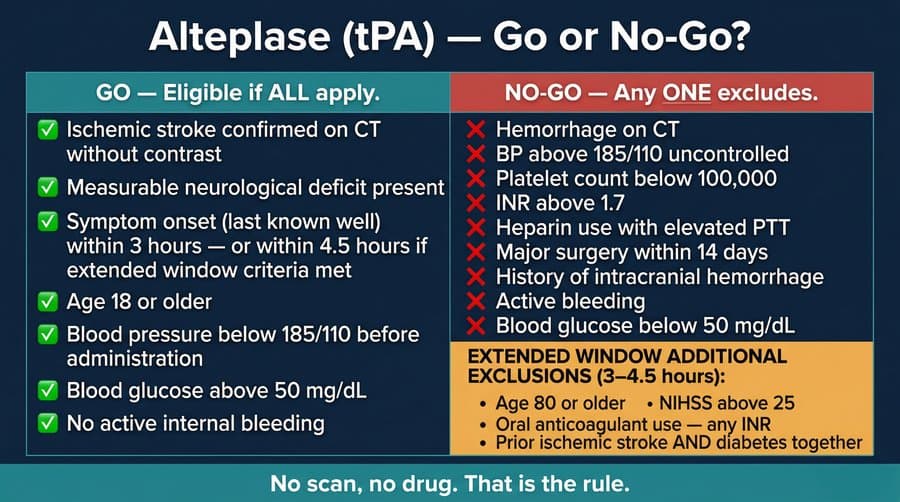
Alteplase is indicated for confirmed ischemic stroke within 3 hours of last known well. The window extends to 4.5 hours in selected patients who meet all inclusion criteria and have no additional exclusions. The standard exclusion criteria include hemorrhage on CT, blood pressure above 185/110 uncontrolled, platelet count below 100,000/mm3, INR above 1.7, recent heparin use with elevated PTT, major surgery within 14 days, history of intracranial hemorrhage, active internal bleeding, and blood glucose below 50 mg/dL.
The extended window from 3 to 4.5 hours adds four specific exclusions: age 80 or older, NIHSS score above 25, current oral anticoagulant use regardless of the INR value, and the combination of prior ischemic stroke plus diabetes mellitus. Either condition alone does not exclude eligibility in the extended window — both together do. This is a commonly tested distinction.
Alteplase Dosing and Administration
The standard dose is 0.9 mg/kg intravenously, with a maximum of 90 mg. Ten percent of the total dose is given as an IV bolus over one minute. The remaining 90% is infused over 60 minutes. The drug requires a dedicated intravenous line and weight-based calculation, with accurate weight measurement critical — overdose increases the risk of intracranial hemorrhage.
Monitoring During tPA Infusion
During alteplase infusion, neurological assessment is performed every 15 minutes. Blood pressure is monitored at the same frequency and must remain below 180/105 mmHg throughout. Any new headache during infusion must be treated as a possible sign of hemorrhagic transformation and requires immediate cessation of the infusion and physician notification. Stopping promptly is essential — no finishing the bag, no waiting for confirmation. Additional warning signs include a decrease in level of consciousness, new asymmetric pupils, or sudden worsening or new neurological deficits.
Post-tPA Care and Aspirin Timing
After alteplase administration, no antiplatelet or anticoagulant therapy is given for 24 hours. Alteplase clears rapidly, with a plasma half-life under 5 minutes, but the vessel walls it acted on require time to restabilize. At 24 hours, repeat non-contrast CT is performed to rule out hemorrhagic transformation. If imaging is clear, aspirin therapy may begin. Initiating antiplatelet therapy before this confirmation increases the risk of microbleeding expanding into a significant hemorrhage.
Mechanical Thrombectomy
For ischemic stroke caused by large vessel occlusion — blockage of the intracranial internal carotid artery, proximal middle cerebral artery, or basilar artery — mechanical thrombectomy is now a recommended treatment option. A catheter is used to physically retrieve the clot. The treatment window extends up to 24 hours from last known well in selected patients with favorable imaging. Alteplase and thrombectomy are not mutually exclusive in eligible patients. When a large vessel occlusion is identified, neurosurgical or interventional neurology consultation should be initiated promptly regardless of tPA eligibility.
Nursing Priorities Post-Stroke
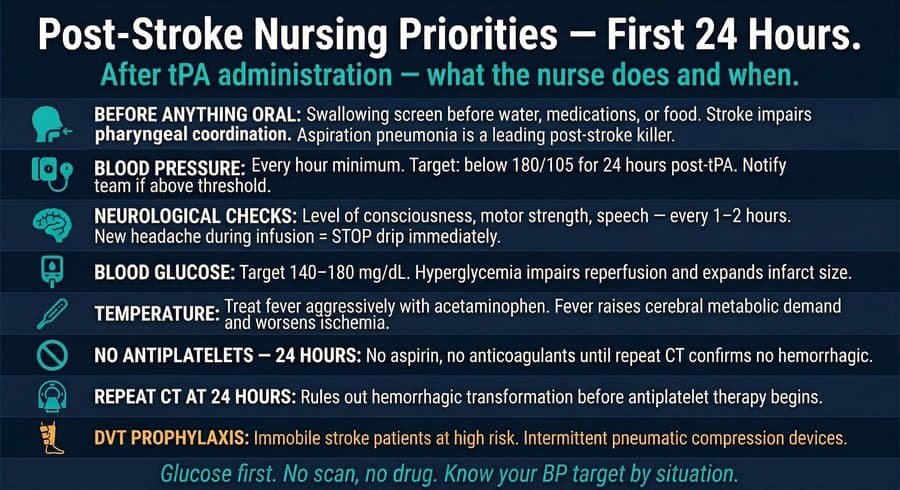
Before any oral intake — water, medications, food, or ice chips — swallowing must be assessed. Stroke frequently impairs pharyngeal muscle coordination, and aspiration may occur even in alert, cooperative patients. Aspiration pneumonia is a leading cause of post-stroke mortality and is preventable with systematic assessment. If speech therapy is not immediately available, a bedside water swallow screen is performed. Any signs of coughing, choking, or wet voice quality following a small sip require that oral intake be withheld until formal evaluation. Oral medications cannot be crushed and administered without a swallowing evaluation; an intravenous alternative must be arranged.
Additional 24-hour monitoring priorities include hourly blood pressure assessment, serial neurological checks for deterioration, blood glucose management targeting 140 to 180 mg/dL (hyperglycemia independently worsens ischemic outcomes by impairing reperfusion), temperature monitoring with aggressive fever treatment using acetaminophen, and deep vein thrombosis prophylaxis for immobile patients using intermittent pneumatic compression. [See Chart 3]
Stroke Mimics
Several conditions present with acute focal neurological deficits that mimic stroke. The most immediately actionable is hypoglycemia. The brain has no meaningful glucose storage and depends entirely on circulating blood sugar. When glucose falls below a critical threshold, sodium-potassium pumps in neurons fail, ion gradients collapse, and focal neurological deficits appear that can precisely mirror a vascular distribution. Treatment is dextrose — not alteplase. For this reason, fingerstick blood glucose is the first action for any patient presenting with new focal neurological deficits, before CT and before the stroke protocol. Other stroke mimics include seizure with postictal deficit, known as Todd paralysis, functional neurological disorders, complicated migraine, and septic encephalopathy.
The clinical sequence is non-negotiable: glucose first, then CT without contrast, then the treatment decision. No scan, no drug. That is the rule.
New episodes drop every week — one topic at a time until you have the whole exam covered.