NCLEX Seizures and Epilepsy — Types, Triggers, Seizure Precautions, and Nursing Care
April 11, 2026
Test Your Knowledge
12 questions · Audio-based · Study on the go
Seizures and Epilepsy: Types, Triggers, Precautions, and Nursing Care
Epilepsy affects approximately 3.4 million people in the United States, and seizure management is one of the most clinically significant areas of neurological nursing. Understanding seizure types, recognizing common triggers, establishing correct seizure precautions, and providing safe care during and after a seizure episode are foundational nursing competencies. Each of these areas contains clinical distinctions that directly affect patient safety and nursing documentation accuracy.
Seizure Classification
The current classification system divides seizures into two major categories: generalized onset and focal onset. Generalized seizures involve abnormal electrical activity distributed across both hemispheres simultaneously from the beginning of the event.
Tonic-clonic seizures, formerly called grand mal seizures, are the most recognizable type. They begin with a tonic phase — a period of sustained muscle stiffening that may produce a brief cry as air moves through the vocal cords — followed by a clonic phase of rhythmic, bilateral jerking. Loss of consciousness occurs. The seizure is followed by a postictal state of confusion, fatigue, and disorientation that may last from minutes to hours.
Absence seizures, formerly called petit mal seizures, are the most frequently underdocumented seizure type in clinical settings. They present as brief episodes of impaired awareness — typically 10 to 30 seconds — during which the patient stares blankly, may blink rapidly, and does not respond to external stimuli. There is no postictal period. The patient returns to full awareness immediately and resumes prior activity without apparent confusion. A key clinical distinction: absence seizures cannot be interrupted by calling the patient's name, touching them, or other stimulation. A nurse who documents this presentation as "brief altered mental status with return to baseline" has missed the diagnosis. Documentation should specify onset time, duration, whether the episode could be interrupted, and the patient's behavioral state immediately following.
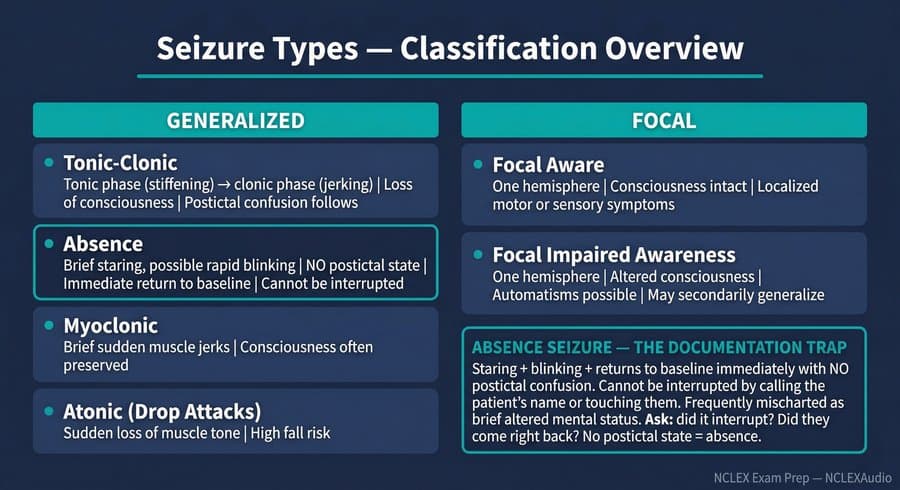
Myoclonic seizures produce brief, sudden muscle jerks that may be unilateral or bilateral, with consciousness often preserved. Atonic seizures, also called drop attacks, involve sudden loss of muscle tone and carry significant fall risk. Focal seizures originate in a single hemisphere. Focal aware seizures preserve consciousness while producing localized symptoms. Focal impaired awareness seizures alter consciousness and may involve automatisms such as lip-smacking or repetitive hand movements. Focal seizures may secondarily generalize to both hemispheres.
Common Seizure Triggers
In patients with established epilepsy, breakthrough seizures occur most commonly when a precipitating factor lowers the seizure threshold. Medication noncompliance is the most prevalent cause. Patients who feel well on antiepileptic therapy sometimes discontinue medication under the mistaken belief that they no longer require it. The therapeutic effect of antiepileptic drugs depends entirely on maintaining consistent serum levels; once levels fall below the therapeutic range, seizure protection is lost.
Other established triggers include sleep deprivation, febrile illness, alcohol use or withdrawal, and electrolyte imbalances. Hypoglycemia deserves particular clinical attention because it can both cause seizures and produce post-ictal-like confusion that is difficult to distinguish from a prolonged postictal state without objective measurement. For any patient presenting with new seizure activity or unusually prolonged post-ictal confusion, a fingerstick blood glucose should be obtained immediately — before assuming the clinical picture is purely epileptic.
Seizure Precautions: Correct Room Setup
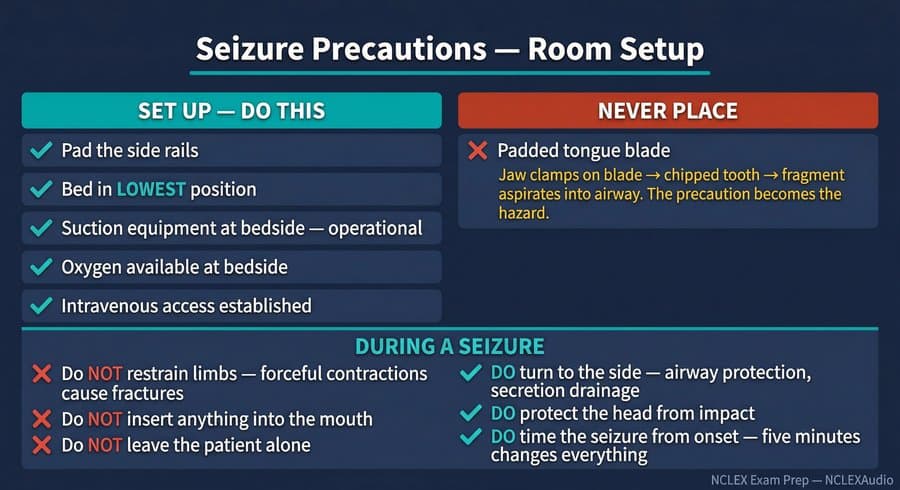
When a patient with a known or suspected seizure disorder is admitted, the nurse initiates seizure precautions as a standard safety measure. The correct precaution setup includes five elements: padded side rails, bed maintained in its lowest position, suction equipment at the bedside and operational, oxygen available at the bedside, and intravenous access established to allow emergency medication administration.
A persistent and clinically dangerous misconception is that a padded tongue blade should be placed at the bedside. This item appears in older clinical training materials, but it is not supported by current practice. The historical rationale was to prevent biting of the tongue or to protect the airway. However, the tongue is anatomically anchored and cannot be swallowed or retract to cause obstruction during a seizure. If a patient bites down on a tongue blade during a tonic-clonic seizure, the force of jaw clenching can fracture the object or chip the surrounding tooth structure. The resulting fragment can enter the airway and cause aspiration. The tongue blade belongs nowhere in a correctly established seizure precaution setup.
Nursing Care During an Active Seizure
When a seizure occurs, the nurse's priorities are lateral positioning, environmental safety, timing, and observation. The patient should be turned to the side to facilitate drainage of secretions and maintain airway patency. Any objects that could cause impact injury should be cleared from the immediate area. If the patient is in bed, padding should protect the head from striking the rails or mattress edge. The nurse remains with the patient throughout.
Nothing should be inserted into the mouth during an active seizure — no tongue blade, no airway adjunct, no fingers. Inserting objects risks dental fracture, jaw injury, and aspiration of fragments.
The patient should not be physically restrained. During tonic-clonic activity, muscle contractions are forceful. Attempting to hold limbs in position against these contractions risks bone fractures and joint injuries. The correct response is to clear the environment, not restrict the movement.
Seizure onset time must be documented from the beginning of the episode. Duration is clinically significant.
Status Epilepticus
Status epilepticus is defined as continuous seizure activity lasting five minutes or longer, or repeated seizures occurring without the patient returning to baseline between episodes. Five minutes is the threshold — not ten, not fifteen. This represents a neurological emergency requiring immediate intervention.
First-line treatment is a benzodiazepine. Lorazepam administered intravenously is preferred when vascular access is established. Intramuscular midazolam is an effective and evidence-supported alternative when intravenous access is unavailable. The benzodiazepine is always administered first — not as a secondary agent after anticonvulsants, and not withheld in favor of reaching for fosphenytoin or levetiracetam. Underdosing benzodiazepines and bypassing them for other agents is a documented contributor to prolonged status epilepticus.
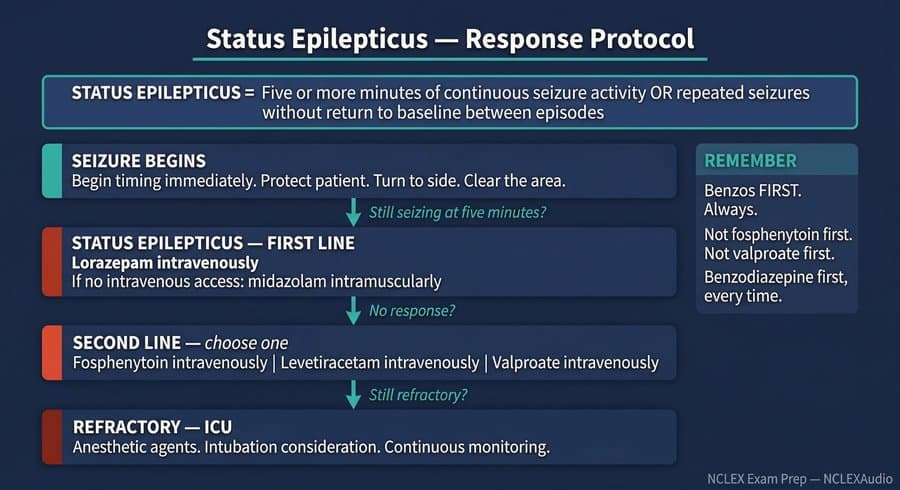
If seizures continue after adequate benzodiazepine dosing, second-line anticonvulsants are initiated: fosphenytoin, levetiracetam, or valproate, each administered intravenously. Refractory status epilepticus requires intensive care unit transfer and anesthetic agents under continuous monitoring.
Post-Ictal Assessment
Following a seizure, structured post-ictal assessment begins with airway confirmation and vital signs. A fingerstick blood glucose is obtained to exclude hypoglycemia as a contributing cause of ongoing confusion. Neurological status is assessed and documented with specificity — level of consciousness, orientation, motor function bilaterally, and speech quality.
A finding that requires careful clinical differentiation from ischemic stroke is post-ictal focal weakness, historically referred to as Todd's paralysis or Todd's paresis. Following a focal or generalized seizure, some patients develop transient weakness in the body region corresponding to the area of maximal cortical activity during the seizure. This weakness appears immediately after the seizure ends and is expected to improve progressively, resolving within minutes to a few hours in most cases, and within 36 hours in the vast majority.
The critical distinction from stroke is timing and trend. Post-ictal focal weakness is present immediately after a witnessed seizure and improves on serial assessment. Serial neurological assessments performed at regular intervals — every 15 minutes is standard — document whether the weakness is trending toward resolution. Improving weakness in a patient with a known seizure event supports a diagnosis of post-ictal weakness. Weakness that fails to improve, worsens, or is accompanied by any new symptom not present in the immediate post-ictal period requires escalation and imaging evaluation.
Documentation
Every seizure event requires specific documentation: onset time, duration, observed characteristics including body areas involved and state of consciousness, and the post-ictal course. Absence seizures require the same documentation specificity as tonic-clonic events. A chart entry that reads "brief unresponsiveness, returned to baseline" is insufficient if the presentation was consistent with an absence episode. Accurate documentation supports correct diagnosis, appropriate medication management, and a usable clinical baseline for future comparison.
New episodes drop every week — one topic at a time until you have the whole exam covered.